Assessing cartilage on MRI can vary from simple to very complicated. In this post we review the standard features of cartilage damage in day to day reporting.
SEQUENCES:
- On a 1.5T or 3T MRI, cartilage is best assessed on PD sequences.
- There is no need to do a volume FLASH or similar volume sequence as it doesnt add any more information and takes extra time.
- If you are using a lower field strength magnet, you need to run both the PD and volume sequences initially to see which one shows cartilage better and then use that for future scans.
PLANES TO ASSESS:
- Assess cartilage in all planes.
- The trochlea and patella cartilage can be more difficult to assess on the axial plane where they curve away from the true axial plane.
- Look at the sagittal scans to assess these areas.

TYPES OF ABNORMALITIES:
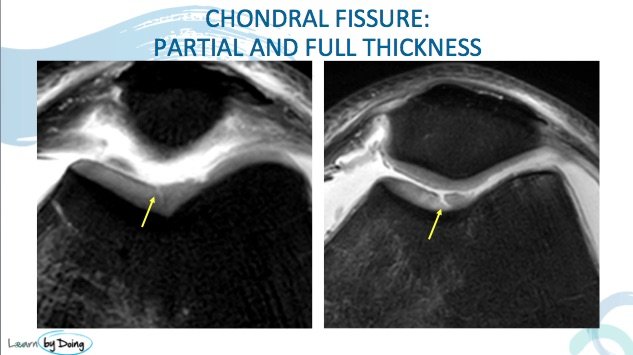
1. FIBRILLATION AND FISSURING:
- Fibrillation is irregularity of the chondral surface.
- It has a hair comb type appearance.

- Fissuring is the next stage where the chondral loss goes deeper and can be partial or full thickness ( down to bone).
- There is no measurement where fibrillation becomes fissuring.
2. FOCAL CARTILAGE LOSS:
- Wider than a fissure and can be partial or full thickness.
- Look for loose bodies.
- When its focal like this give measurements of width and depth in your report.


3. GENERALISED THINNING AND FULL THICKNESS CARTILAGE LOSS:
- This is chondral loss over a greater area and not focal.
- In your report give an indication of the severity ( mild/moderate/severe/complete) and the extent of the surface involved.
 Image Above: Red arrow generalised severe thinning of cartilage . Yellow arrows full thickness cartilage loss.
Image Above: Red arrow generalised severe thinning of cartilage . Yellow arrows full thickness cartilage loss.
4. LOOSE BODIES:
- Dont forget to look for cartilage loose bodies.
- Usually they will have a similar appearance to normal cartilage.
